MST Markers: What They Are and How a Psychologist Reads Them
- 1.What are MST markers?
- 2.What counts as a marker? Three groups
- 3.How a psychologist reads markers
- 4.How the courts locked this in: Menegassi and AZ
- 5.Why marker-based claims still get denied
- 6.What if my claim was already denied?
- 7.Do you need every marker?
- 8.Get a clinician-built marker review
- 9.Frequently asked questions
Most military sexual trauma was never reported. The VA knows this, and it built the claims rules around it. If you experienced MST and never told anyone in an official capacity, your claim does not depend on a report that was never filed. It depends on markers, and on how well someone finds and explains them.
That second part is what this article is really about. In MST claims the explanation matters more than in any other claim type, for a reason we will get to.
The Short Answer
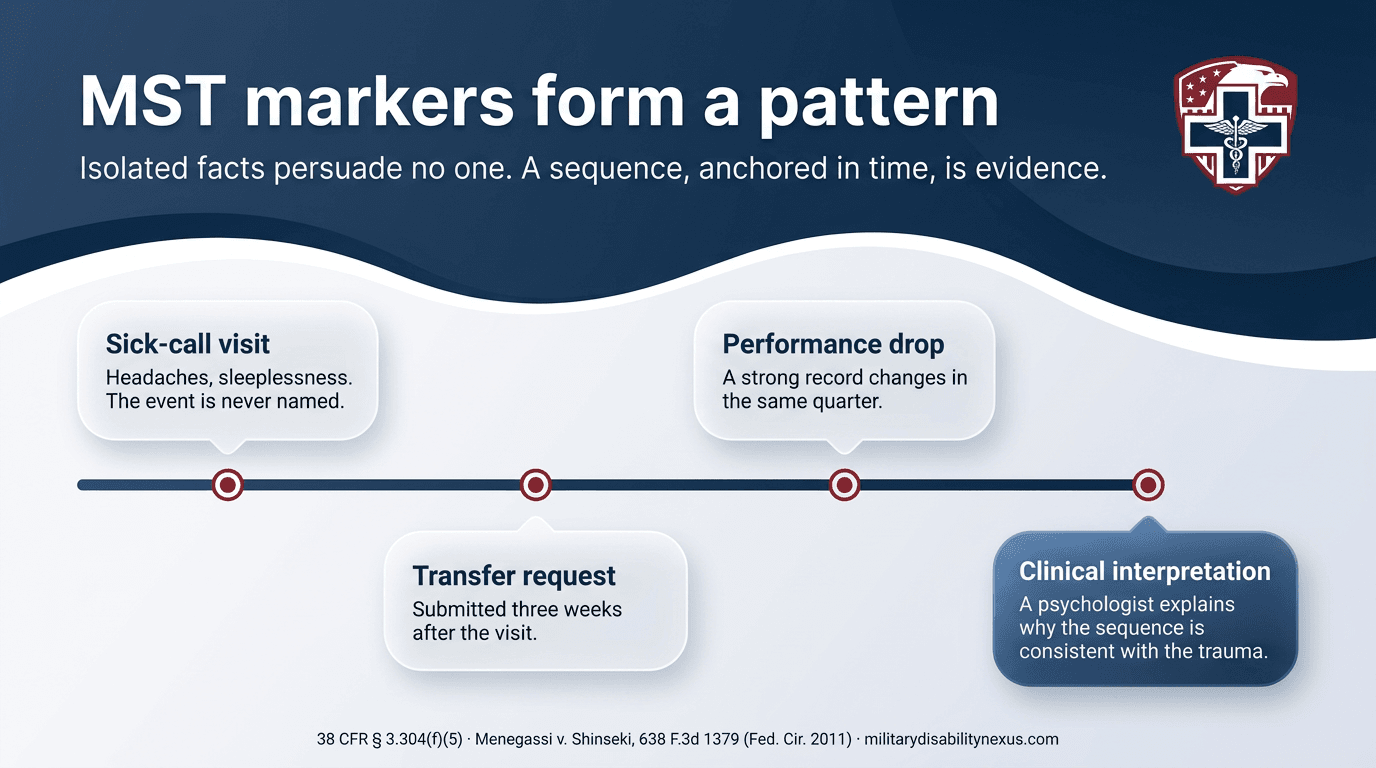
MST markers are the indirect evidence the VA accepts to support a military sexual trauma claim when the event was never officially reported: records from the time, changes in a veteran's service record, and statements from people who knew. Under 38 CFR § 3.304(f)(5), a qualified clinician's written interpretation of the markers can help corroborate that the event occurred. The pattern, explained well, is the evidence.
What are MST markers?
Markers are the traces a traumatic experience tends to leave behind, even when the event itself was never documented. The regulation, 38 CFR § 3.304(f)(5), names them directly: records from law enforcement, rape crisis centers, mental health counseling, or medical providers, tests for pregnancy or sexually transmitted infections, statements from family members, roommates, fellow service members, or clergy, and evidence of behavior changes such as a request for transfer, deterioration in work performance, substance abuse, or unexplained changes in social and economic behavior.
The rule exists because the VA recognized a reality that survivors already knew. Reporting was rare, and punishing claims for the absence of a report would have punished veterans for the very silence the trauma imposed. MST affects veterans of every gender, and because most veterans are men, a large share of those who disclose MST to the VA are men, many of them speaking for the first time decades after service.
What counts as a marker? Three groups
In our record reviews, markers fall into three broad groups. A claim rarely needs all of them. It needs the ones that exist, found and explained well.
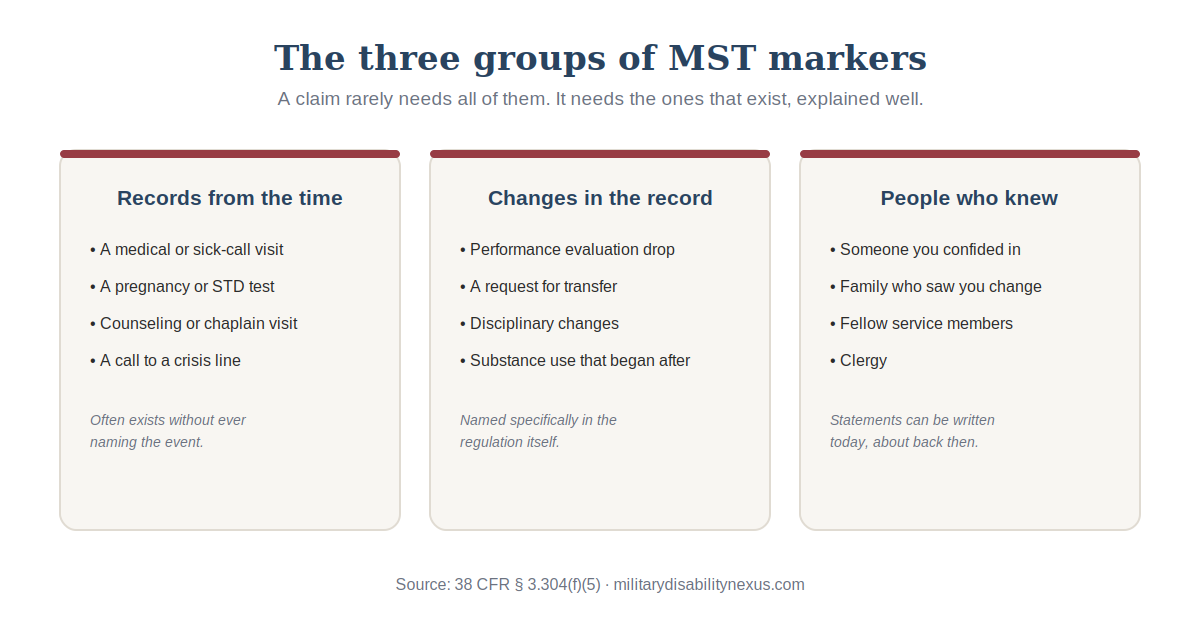
1. Records from the time
A medical visit, a pregnancy or STD test, a session with a counselor or chaplain, or a call to a crisis line. These records often exist without ever naming the event. A sick-call visit for headaches and sleeplessness three days after the assault names no assault, yet its timing may be part of the pattern.
2. Changes in the service record
A drop in performance evaluations, a request for transfer, disciplinary problems that appeared out of nowhere, or substance use that began after a certain point. The regulation names these specifically, because a sudden change in a previously strong record is evidence in itself.
3. People you told, or who noticed
A statement from someone you confided in at the time, or from family and friends who watched you change, is competent evidence the VA must consider. These statements can be written today about what was seen and heard then, even decades later.
How a psychologist reads markers
Here is where MST claims differ from every other claim type, and where most of them are won or lost.
For an ordinary PTSD stressor, a clinician's opinion does one job. It connects an already verified event to the current diagnosis. In MST claims, the rules allow something more. The VA may rely on a qualified clinician's interpretation of the marker evidence to help corroborate that the event itself occurred. The opinion can matter twice, once for the stressor and once for the nexus. No other stressor type works this way.
What does that interpretation actually involve? Three things, in our practice.
1. Timeline anchoring
Isolated facts persuade no one. A transfer request means little to a rater as a line item. A transfer request submitted three weeks after a sick-call visit, in the same quarter a previously excellent performance record dropped, is a sequence. The clinician's job is to lay that sequence out plainly, with dates, so the pattern is visible on paper rather than left for the rater to assemble.
2. Consistency with the clinical literature
Trauma responses follow recognizable patterns: avoidance of the location or the people involved, sudden social withdrawal, new substance use, deteriorating performance without another explanation. A psychologist can state, in writing, that the documented pattern is consistent with the known behavioral aftermath of sexual trauma, and can address the alternative explanations a rater might reach for. That sentence, properly supported, is what turns a coincidence into corroboration.
3. Connecting the pattern to the present diagnosis
The final step is the nexus itself: a structured diagnostic evaluation confirming the current condition, and a written opinion connecting the corroborated stressor to it under the "at least as likely as not" standard. The rating that follows depends on documented occupational and social impairment, which we cover in depth on our PTSD nexus letter page.
How the courts locked this in: Menegassi and AZ
The double-duty role of the clinician's opinion is not our theory. It is settled federal case law, and two decisions carry it.
Menegassi v. Shinseki, 638 F.3d 1379, 1382 (Fed. Cir. 2011)The Federal Circuit held that under 38 CFR § 3.304(f)(5), medical opinion evidence may be submitted for use in determining whether the occurrence of the stressor is corroborated. In plain terms, a qualified clinician's opinion, even an examination performed many years after the assault, can itself help establish that the event happened. That is the double duty this article describes, written into binding precedent.
AZ v. Shinseki, 731 F.3d 1303 (Fed. Cir. 2013)The The Federal Circuit addressed the other side of the coin: the missing report. Because sexual assault in service so often goes unreported, the absence of a report in the service records is not evidence that the assault did not occur. The VA cannot treat your silence at the time as proof against you.
The Board applies these holdings in real decisions. In a December 2023 case, Citation Nr. 23066710, the Board found the regional office's handling of an in-service personal assault claim contrary to Menegassi and § 3.304(f)(5), and credited examiner opinions that supported the veteran's reported stressor. The pattern in these decisions is consistent: the denial treats each marker as an isolated fact, and the grant comes when a clinician connects them and the Board weighs that interpretation as the corroboration the regulation invites.
Why marker-based claims still get denied
Approval rates for MST-related PTSD claims have improved substantially over the past decade, yet denials remain common, and in our reviews they usually trace to one of three gaps.
The markers were never gathered. Personnel files, old medical records, and the memories of people who were there hold most of the evidence, and most denied claims were filed without a systematic search of any of it. The VA rated the silence.
The markers were listed, not interpreted. A claim that attaches a transfer request and a performance drop without explanation asks the rater to do the clinical reasoning. Raters are not clinicians, and the rules do not require them to connect the dots. The written interpretation is the connecting, and most claims never include one.
The impairment was never documented. Service connection is half the claim. The rating follows how symptoms affect work and daily life, and a file that proves the stressor but stays silent on functioning gets rated low. Our mental health claims page explains how the rating formula measures function rather than diagnosis.
What if my claim was already denied?
Often the denial is where the real work starts. Many older denials predate today's application of the marker framework, and many failed simply because no one gathered or interpreted the evidence. A denial, even one from the legacy system years ago, can be revisited through a Supplemental Claim with new and relevant evidence, and a marker-based record review with a clinician's written interpretation is frequently exactly that evidence. Be aware that benefits granted this way generally date from the new filing rather than the original claim. An accredited representative can advise on effective-date questions.
Do you need every marker?
No. We have seen claims carried by two markers and a well-written lay statement, and we have seen claims with more evidence fail because none of it was explained. The question is never how many boxes are checked. It is whether the pattern that exists has been found, anchored in time, and interpreted by someone qualified to say what it means. If you are not sure what your records hold, that is a normal place to start, and finding out commits you to nothing.
Get a clinician-built marker review
Our licensed psychologists perform the systematic marker review, the written clinical interpretation, and a private diagnostic evaluation at your pace, with your choice of clinician gender accommodated wherever possible. That is the whole service, described plainly on our MST-related PTSD nexus letter page.
Frequently asked questions
What are examples of MST markers?
Common examples include a medical visit, pregnancy test, or STD test around the time of the event, a session with a counselor or chaplain, a sudden drop in performance evaluations, a request for transfer, disciplinary changes in a previously clean record, substance use that began after a certain point, and statements from family, friends, fellow service members, or clergy who were told at the time or who noticed the change.
Can the VA deny an MST claim if there are no markers?
A claim without any supporting evidence is difficult, but the absence of obvious markers is not the end. Markers are often missed rather than missing, sitting in records nobody requested or in the memory of someone never asked. A veteran's own detailed statement is also evidence, and lay statements can be written today about what was seen and heard then. A systematic review frequently finds support the original claim never gathered.
Who can write a buddy statement for an MST claim?
Anyone with firsthand knowledge. Someone you confided in at the time, a family member who watched you change during or after service, a fellow service member who noticed the shift, or clergy. The statement describes what they were told and what they observed, and it can be written today about events from decades ago.
Do markers prove the assault happened?
Markers are indirect evidence, and no single marker proves anything by itself. Their power is in the pattern, and in MST claims specifically, the VA may rely on a qualified clinician's written interpretation of that pattern to help corroborate that the event occurred. That clinical interpretation is unique to MST claims and is often the difference between a file the VA reads as coincidence and a file it reads as evidence.
Do male veterans file MST claims?
Yes. MST affects veterans of every gender, and because most veterans are men, a large share of the veterans who disclose MST to the VA are men. The marker rules, the claim process, and the evaluation process are the same, and many male veterans file decades after service, having never told anyone.
My MST claim was denied years ago. Can markers help now?
Often yes. Many older denials predate today's application of the marker framework, and many failed because no one gathered or interpreted the marker evidence. A denial can be revisited through a Supplemental Claim with new and relevant evidence, and a marker-based record review with a clinician's written interpretation is frequently exactly that evidence. Be aware that benefits granted this way generally date from the new filing rather than the original claim. An accredited representative can advise on effective-date questions.
Need help with your VA claim?
Get expert guidance and documentation from our licensed clinicians
Get Free ConsultationDr. Kishan Bhalani is a subject matter expert on VA disability claims documentation, with more than five years of focused work at the intersection of clinical m…
Dr. Kishan Bhalani is a subject matter expert on VA disability claims documentation, with more than five years of focused work at the intersection of clinical m…
Originally published July 14, 2026 • Last updated July 14, 2026
Related Insights
PTSD VA Disability Claim: Nexus Letters, Denial Reasons & Your Complete Filing Guide
Can PTSD Cause Migraines? The Clinical Case for Migraines Secondary to PTSD
Who Should Write Your VA Nexus Letter? A Clinician's Specialty-by-Specialty Guide (2026)
About this article. This post is general educational and medical information published by the Military Disability Nexus clinical team. It is not legal advice, not individualized medical advice, and not a substitute for a personal evaluation by a licensed clinician or a consultation with an accredited representative. Reading it does not create a doctor-patient or attorney-client relationship. VA law and rating criteria change; some details may not reflect the most recent updates, and every claim is decided by the VA on its own facts – no outcome is promised or guaranteed. Military Disability Nexus is an independent medical-evidence provider and is not affiliated with, endorsed by, or acting on behalf of the U.S. Department of Veterans Affairs or any government agency. Free claims assistance is available from VA-accredited Veterans Service Organizations and county Veterans Service Officers; you can verify any representative's accreditation through the VA Office of General Counsel.