Can PTSD Cause Migraines? The Clinical Case for Migraines Secondary to PTSD
- 1.How PTSD actually triggers migraines
- 2.What the research shows
- 3.How the VA rates migraines once they're connected
- 4.Direct, secondary, or aggravated: Pick the Right Lane
- 5.real board decisionHow one veteran won his migraine claim in 2025
- 6.What a strong PTSD-to-migraine nexus letter has to show
- 7.Get a clinician-built nexus letter for your migraine claim
- 8.Frequently asked questions:
- 9.Sources
Law firms tell you the legal rule. Here we show you the biology — the actual stress-hormone pathway that connects post-traumatic stress to migraine attacks, and what the VA needs to see in writing.
If you have a service-connected PTSD rating and you also get migraines, you may be able to claim those migraines secondary to PTSD - meaning the VA pays for them as a condition your PTSD caused or made worse. This is one of the most winnable secondary claims when the evidence is built correctly, and one of the most commonly denied when it isn't. The difference is almost never the law. It's the medical explanation. Below is the mechanism a strong nexus letter has to spell out, the rule the VA uses to rate migraines, and a real 2025 Board of Veterans' Appeals decision that turned on exactly this argument.
The Short Answer
Yes. The medical literature supports a real biological link between PTSD and migraine. The VA does not presume it, so you have to prove it for your specific case - a current migraine diagnosis, a service-connected PTSD rating, and a medical opinion that connects the two with a clear rationale..
How PTSD actually triggers migraines
Migraine is not "just a bad headache." It is a neurological disorder — the brain becomes overly excitable, pain pathways fire abnormally, and blood vessels and brain chemistry react in ways that produce throbbing pain, light and sound sensitivity, nausea, and visual changes. PTSD acts on several of the same systems. That overlap is the heart of the secondary connection.
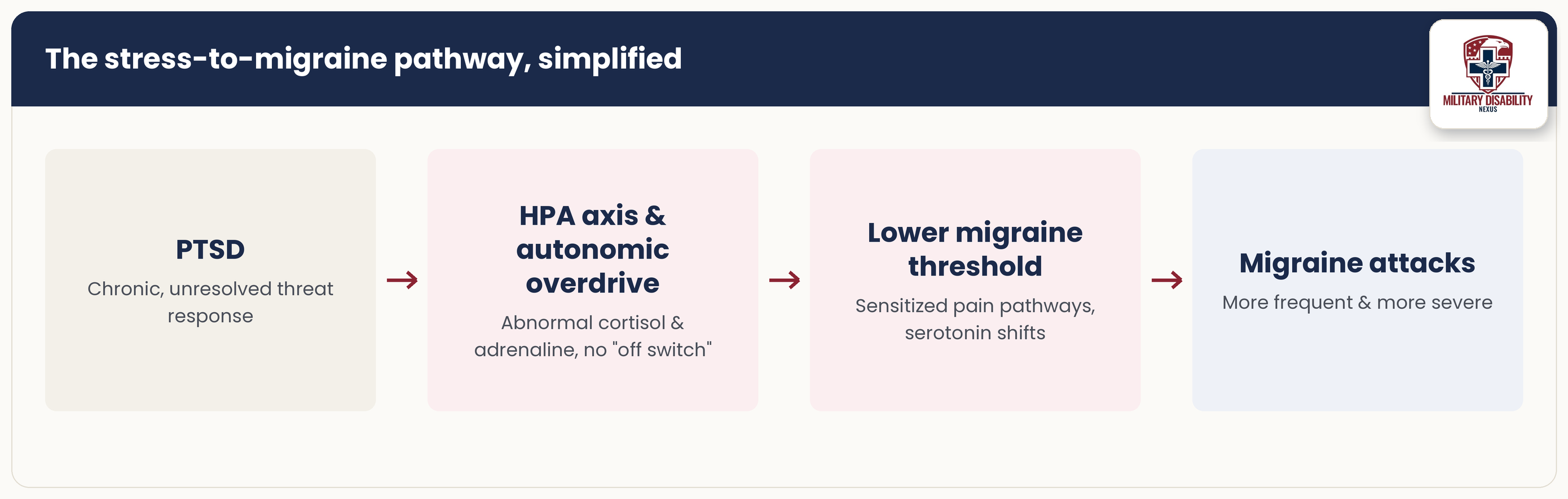
1. The HPA axis stays switched on
Your body has a built-in stress-response chain called the hypothalamic-pituitary-adrenal (HPA) axis. In a healthy system it ramps up during a threat, then ramps back down. In PTSD it doesn't reset properly. The result is a long-running pattern of abnormal stress hormones: cortisol and adrenaline that don't follow their normal daily rhythm. That constant chemical stress lowers the threshold at which a migraine fires. The brain, in effect, sits closer to the edge all the time. This is the single most important mechanism to name in a nexus letter, and it is the one a clinician can defend with published evidence.
2. The autonomic nervous system tips toward "fight or flight"
PTSD pushes the autonomic nervous system — the part that runs heart rate, blood vessels, and the stress reflex into a state of overdrive. Researchers measure this as reduced heart rate variability and a persistently elevated stress response. People who get migraines show similar autonomic instability. When both conditions pull the same lever, attacks come more easily.
3. Serotonin and brain chemistry overlap
Both PTSD and migraine involve disrupted serotonin signaling. Serotonin helps control pain pathways and the tone of blood vessels in the brain. That shared chemistry is one reason a single medication certain antidepressants - is sometimes used to treat both. Shared biology is also why these conditions cluster together rather than appearing at random.
4. Stress sensitizes the pain system over time
Chronic stress and chronic pain can "train" the nervous system to be more reactive, a process clinicians call central sensitization. Over months and years, the migraine threshold drops and attacks that were occasional become frequent. This is why a veteran can have mild or rare headaches early on, then a clear worsening once PTSD takes hold — a pattern the VA recognizes as aggravation.
5. The indirect route: PTSD wrecks sleep, and poor sleep triggers migraines
Even setting the brain chemistry aside, PTSD causes chronic sleep impairment — and chronic sleep impairment is one of the listed symptoms the VA uses to rate PTSD itself. Disrupted sleep is one of the best-documented migraine triggers there is. So there is a clean, common-sense chain: PTSD → poor sleep → more migraines. That indirect pathway is often the easiest one for a VA reviewer to accept, and it can stand alongside the direct HPA-axis argument.
What the research shows
This isn't a fringe theory. A foundational review in the journal Headache laid out the epidemiology and the leading mechanisms: HPA-axis dysfunction, autonomic changes, and serotonin involvement — behind the PTSD–migraine link. Population data back it up: people with migraine carry PTSD at rates several times higher than people without headache, and in the majority of people who have both, the PTSD symptoms came first — the timeline you'd expect if PTSD were driving the headaches rather than the reverse. More recent work, including a large bidirectional study in nurses and genetic studies in twins, confirms the two conditions are strongly and biologically linked rather than merely coincidental. For a nexus letter, that body of evidence is the difference between an opinion that reads as a hunch and one that reads as medicine.
How the VA rates migraines once they're connected
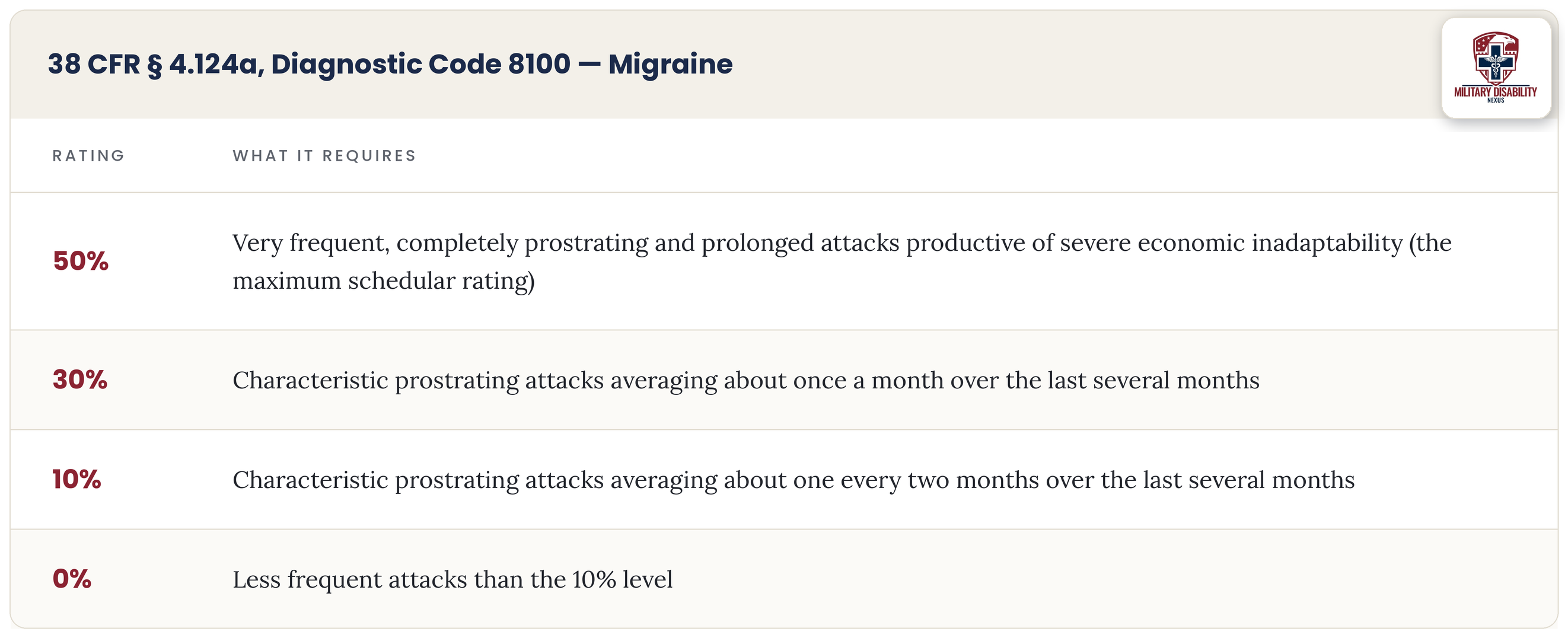
Migraines are rated under 38 CFR § 4.124a, Diagnostic Code 8100. The rating ladder turns almost entirely on how often you have prostrating attacks - attacks so severe you have to stop what you're doing and lie down and how much they interfere with work.
Two practical points the VA's own manual and the courts have confirmed: the rating looks at all your migraine symptoms - nausea, light sensitivity, dizziness not only the head pain; and you don't have to be completely unemployable to reach 50%. Because the whole ladder is built on frequency, anything that increases how often you get prostrating attacks directly affects your rating. Hold onto that idea — it is exactly what won the case below.
Direct, secondary, or aggravated: Pick the Right Lane
There are three ways to connect migraines to service, and a good claim often argues more than one:
Direct service connection means the migraines started in service or are otherwise tied to an in-service event. Secondary service connection (38 CFR § 3.310(a)) means your service-connected PTSD caused the migraines. Aggravation (38 CFR § 3.310(b)) means you had migraines already, but your PTSD made them measurably worse. For migraines, aggravation is powerful, because "worse" usually means "more frequent" and frequency is what the rating is built on.
real board decisionHow one veteran won his migraine claim in 2025
Board of Veterans' Appeals · Citation Nr. A25023065 · Docket No. 240325-427876 · Decided March 12, 2025
An Army veteran with a service-connected PTSD rating filed for migraines as secondary to that PTSD. He described what most veterans with both conditions describe: his headaches hit hardest when his PTSD symptoms — stress, panic, mood swings — were at their worst, and during attacks he had light and sound sensitivity, nausea, dizziness, and throbbing pain.
The VA examiner said no — and undercut his own opinion
The VA's September 2022 examiner gave a negative opinion, stating that PTSD does not directly cause migraines. But in the same breath, he admitted that PTSD can increase how often migraines occur, and pointed to the veteran's insomnia and sleep apnea as additional reasons for the headaches.
The private opinion explained the mechanism
A private clinician submitted an opinion that did the thing VA examiners so often skip: it explained how. Citing the medical literature, it described the prolonged, elevated stress response of PTSD activating the HPA axis, releasing abnormal cortisol and adrenaline, and producing the hypothalamic dysfunction that drives headaches — concluding the migraines were at least as likely as not due to the veteran's PTSD.
The Board granted the claim. It found the private opinion persuasive because it was grounded in a real rationale and the medical literature. Then it turned the VA examiner's own words against the denial: because Diagnostic Code 8100 rates migraines by frequency, conceding that PTSD "can increase their frequency" is, by definition, conceding aggravation. The Board also noted the veteran's PTSD-driven insomnia and his separately service-connected sleep apnea as further causal links. Resolving reasonable doubt in the veteran's favor, service connection was granted.
The lesson is not subtle. The denial leaned on a label "not a direct cause." The grant came from a clinician who explained the biology and from a Board that understood frequency is the rating. Mechanism beat conclusion.
What a strong PTSD-to-migraine nexus letter has to show
Here is what the evidence needs to establish and why each piece matters before you file:
A current, documented migraine diagnosis. Without a present disability there is nothing to connect.
Your service-connected PTSD rating, named as the primary condition the migraines flow froml.
A medical opinion using the "at least as likely as not" standard — meaning a 50% or better probability, the threshold the VA requires.
An explained mechanism, not just a conclusion: the HPA-axis and autonomic pathway, and where relevant the sleep pathway, written out in plain clinical terms..
At least one peer-reviewed citation supporting the mechanism, so the opinion reads as medicine rather than opinion.
If your migraines pre-date your PTSD, an aggravation argument showing they became more frequent or severe after PTSD set in.
If you've already been denied, you are not out of options - the case above started with a negative VA exam. A supplemental claim or a Higher-Level Review with a well-built private opinion is the standard path to reverse exactly this kind of denial.
Get a clinician-built nexus letter for your migraine claim
Our medical team writes opinions that explain the mechanism the VA wants to see — with the literature, the rationale, and the rating logic built in. If you have PTSD and migraines, let's look at whether your evidence is ready.
Frequently asked questions:
Will the VA presume my migraines are caused by PTSD?
No. There is no presumption that links the two. You have to prove the connection for your own case with a current diagnosis and a medical opinion. The good news is that the supporting science is strong, which makes a well-built opinion persuasive.
What if my migraines started before my PTSD?
You can still connect them through aggravation under 38 CFR § 3.310(b). If your PTSD made your migraines more frequent or more severe, the VA can award compensation for that worsening. Because migraines are rated by how often prostrating attacks occur, an increase in frequency is exactly the kind of aggravation the rating recognizes.
How high can a migraine rating go?
The maximum schedular rating under Diagnostic Code 8100 is 50%, for very frequent, completely prostrating, prolonged attacks that significantly interfere with work. You do not have to be fully unemployable to qualify for 50%. If your migraines and other conditions keep you from working, you may also explore TDIU.
My VA C&P examiner said PTSD doesn't cause migraines. Is the claim dead?
Not necessarily. As the 2025 Board decision shows, a negative VA opinion can be outweighed by a private opinion that explains the mechanism — and an examiner who admits PTSD increases migraine frequency may have conceded aggravation without realizing it. A supplemental claim with stronger evidence is the usual next step.
What is a "prostrating" attack?
A prostrating migraine is one severe enough that you have to stop what you're doing and lie down or rest until it passes, because of extreme exhaustion or incapacity. How often these occur is the main factor in your rating, so tracking them in a headache journal is worth doing before a C&P exam.
Sources
Bidirectional analysis of the association between migraine and PTSD, Nurses' Health Study II. PubMed 2024. PMC11669816;
Mehta D, et al. Monozygotic twin study of shared genes in PTSD and migraine. PMC8258453
Board of Veterans' Appeals, Citation Nr. A25023065, Docket No. 240325-427876 (March 12, 2025). va.gov
38 CFR § 4.124a, Diagnostic Code 8100 (Schedule of ratings — neurological conditions). eCFR
Need help with your VA claim?
Get expert guidance and documentation from our licensed clinicians
Get Free ConsultationDr. Kishan Bhalani is a subject matter expert on VA disability claims documentation, with more than five years of focused work at the intersection of clinical m…
Dr. Kishan Bhalani is a subject matter expert on VA disability claims documentation, with more than five years of focused work at the intersection of clinical m…
Originally published June 21, 2026 • Last updated July 14, 2026
Related Insights
MST Markers: What They Are and How a Psychologist Reads Them
Crohn's Secondary to PTSD VA Claim: Why It Gets Denied
Who Should Write Your VA Nexus Letter? A Clinician's Specialty-by-Specialty Guide (2026)
About this article. This post is general educational and medical information published by the Military Disability Nexus clinical team. It is not legal advice, not individualized medical advice, and not a substitute for a personal evaluation by a licensed clinician or a consultation with an accredited representative. Reading it does not create a doctor-patient or attorney-client relationship. VA law and rating criteria change; some details may not reflect the most recent updates, and every claim is decided by the VA on its own facts – no outcome is promised or guaranteed. Military Disability Nexus is an independent medical-evidence provider and is not affiliated with, endorsed by, or acting on behalf of the U.S. Department of Veterans Affairs or any government agency. Free claims assistance is available from VA-accredited Veterans Service Organizations and county Veterans Service Officers; you can verify any representative's accreditation through the VA Office of General Counsel.