Asthma VA Rating Explained: How DC 6602 Actually Works (And Why a Normal Breathing Test Doesn't Cap Your Rating)
Competitors list the rating table. Here we show you the part they skip: how a single daily inhaler can meet the 30% criteria on its own, even when your breathing test comes back normal.
Most veterans researching their asthma VA rating find the same thing: a table of FEV-1 percentages copied out of the regulation, with no explanation of how raters actually apply it. So they walk into the C&P exam believing the rating lives or dies on a breathing test.
It doesn't. Diagnostic Code 6602 runs on two independent tracks, pulmonary function numbers on one side and treatment requirements on the other, and a single small word connects them. Understanding that word is often the difference between a veteran who accepts 10% and a veteran who realizes their daily inhaler already meets the 30% criteria.
The Short Answer
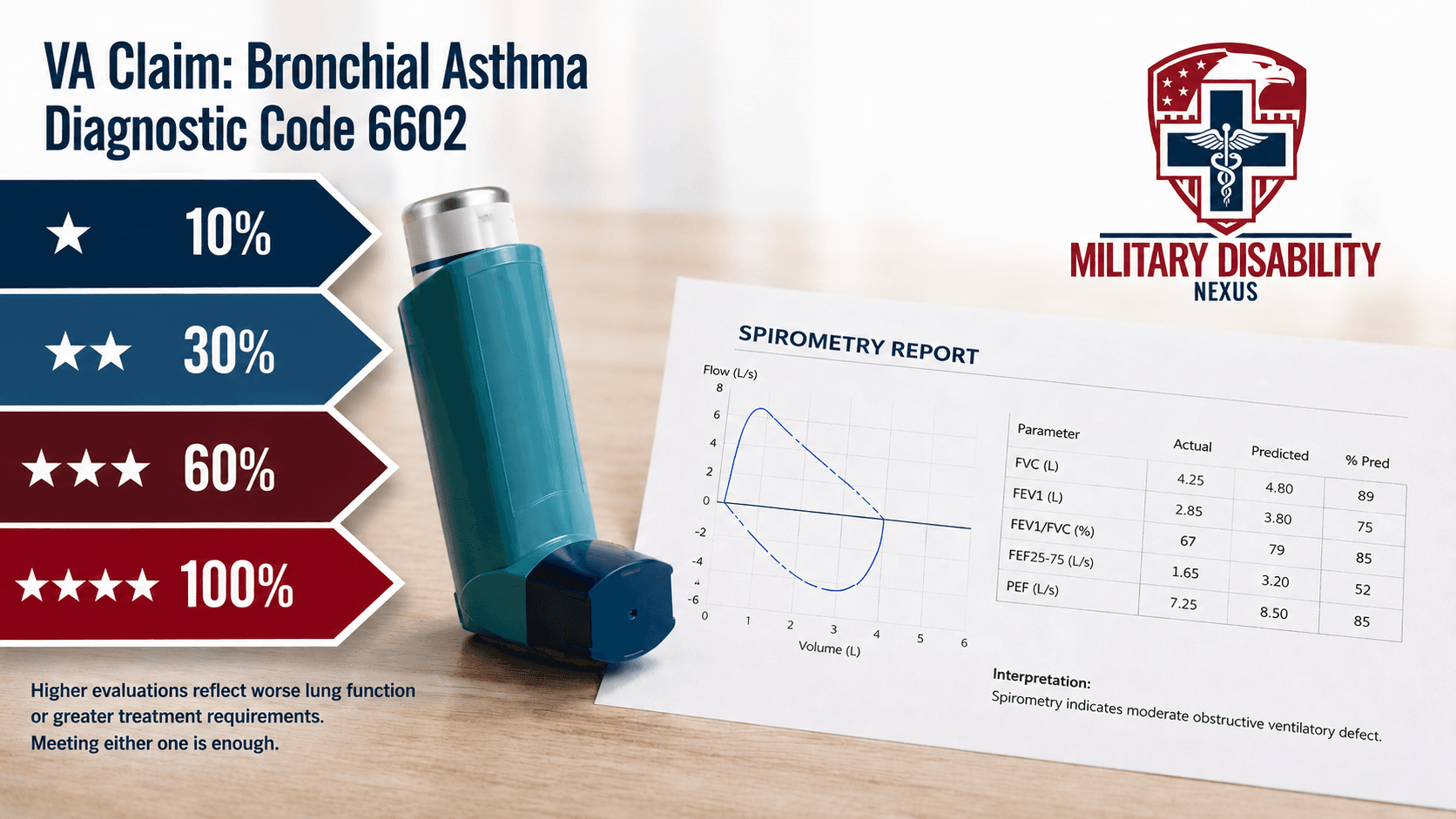
The VA rates asthma under 38 CFR § 4.97, Diagnostic Code 6602, at 10%, 30%, 60%, or 100%. Every tier is written with the word "or," which means you only need to meet one criterion at each level, not all of them. That is why your prescription bottle often matters more than your spirometry printout. Daily use of an inhaled anti-inflammatory medication like Symbicort, Advair, or Flovent meets the 30% criteria on its own, even when your breathing test comes back normal. Documented prednisone bursts at least three times a year meet the 60% criteria the same way.
How DC 6602 rates asthma
Asthma (bronchial asthma) is rated under 38 CFR § 4.97, Diagnostic Code 6602. Here are the four tiers as written, with each independent pathway separated. Within every tier, the pathways are joined by "or." One is enough.
One more scenario. If none of the 10% criteria are documented, the VA can assign 0% under 38 CFR § 4.31. Service-connected, but not compensable. A 0% rating still matters, because the connection is established and the door stays open if your treatment escalates later.
Why your inhaler matters more than your breathing test
Here is the clinical reality behind the regulation: treated asthma often produces normal spirometry. That is what successful treatment is supposed to do.
Asthma is a chronic inflammatory airway disease. Modern management is built around daily inhaled corticosteroid therapy precisely because controlling the inflammation prevents the airflow obstruction a breathing test would otherwise catch. The rating schedule accounts for this. Unlike many diagnostic codes, DC 6602 builds the medication requirement directly into the criteria.

The point most veterans never get told: a veteran on daily Symbicort with an FEV-1 of 95% predicted is not a 0% case. The daily inhaled anti-inflammatory medication is itself the 30% criterion. A normal number is evidence the medication is working, not evidence the disease is gone.
Many low ratings come from exactly this gap. A C&P examiner records excellent pulmonary function results, the rating decision leans on the numbers, and the medication pathway never gets analyzed. If your decision letter discusses your FEV-1 but never mentions your prescription history, you got a rating built on half the criteria.
What counts at each medication tier
Since the medication pathways decide most asthma ratings in practice, precision helps. This is how common evidence maps onto the schedule.
Evidence in your record | Rating pathway it supports |
|---|---|
Albuterol rescue inhaler, used as needed | 10%: intermittent bronchodilator therapy |
Daily controller inhaler: an inhaled corticosteroid (Flovent, Qvar, Pulmicort, Arnuity) or ICS/LABA combination (Symbicort, Advair, Breo, Dulera) | 30%: daily bronchodilator therapy or inhalational anti-inflammatory medication |
Prednisone or Medrol taper courses, at least three per year, dated | 60%: intermittent systemic corticosteroids |
Monthly physician visits required for exacerbation care | 60%: physician-visit pathway |
Daily high-dose oral corticosteroids or immunosuppressive medication | 100% |
1. Your pharmacy records are rating evidence
A prescription written once and never refilled reads as "intermittent." A controller inhaler refilled every 30 days for two years reads as daily use. Refill history is one of the most objective severity documents in your file. Make sure it is actually in the file.
2. Prednisone bursts must be documented, not remembered
Telling an examiner you have needed steroids a few times a year carries little weight. Three dated prescriptions in twelve months is a 60% pathway. The catch: flares often get treated at urgent care or a civilian ER, and those records never reach your VA file unless you submit them.
3. Biologics are a developing question
Veterans on injectable biologics for severe asthma, such as omalizumab (Xolair), mepolizumab (Nucala), or dupilumab (Dupixent), often ask whether these count as "immunosuppressive medications" under the 100% criteria. Board decisions have gone in different directions, and outcomes frequently turn on how the prescribing physician characterizes the medication in the record. If you are on a biologic, that is exactly the kind of question a well-reasoned independent medical opinion should address head-on rather than leave to the rater.
A Real Board decision: when the medication pathway is missing
The clearest way to see why the medication pathway matters is a case where it was absent.
Real Board decision
BOARD OF VETERAN APPEALS · CITATION NR. A25027831 · DECIDED MARCH 25, 2025
An Army veteran who served from 2009 to 2014 was granted service connection for asthma and rated at 10% back to August 2022. He appealed, arguing the rating understated how much the condition affected him.
What the record actually showed
The evidence documented intermittent bronchodilator use. It did not document the next rung: daily inhalational or oral bronchodilator therapy, or a daily inhaled anti-inflammatory medication, the pathway that defines 30%. His FEV-1 values also sat in the range the schedule ties to 10%.
Why the Board could not go higher
Because DC 6602 is written in the "or" structure, the Board looks for any single 30% pathway to be met. Here, neither the numbers nor the documented medication reached it. The Board denied the increase above 10%, holding the higher criteria were not more nearly approximated.
The lesson is not that the veteran wasn't sick enough. It is that the file never established which pathway he met. If a daily controller inhaler existed but was never documented and argued as the 30% criterion, the record the Board reviewed would not show it. The rating follows what is in the file, not what is in the medicine cabinet.
The rating follows your file, not your medicine cabinet.
The spirometry side: FEV-1 and FEV-1/FVC
The numeric pathway still matters, especially at the higher tiers, so here is what the two numbers mean. FEV-1 (forced expiratory volume in one second) measures how much air you can force out in the first second of a hard exhale, as a percentage of what is predicted for your age, height, and sex. FEV-1/FVC is the ratio of that one-second volume to your total forced exhale, and a reduced ratio is the signature of obstructive disease.
Two things to know before your pulmonary function test.
Asthma fluctuates. A test performed during a good stretch understates your baseline disease. If you recently recovered from a flare or took your medications shortly before testing, say so. That timing context belongs in the report.
Bring your history anyway. Because the medication and exacerbation pathways stand on their own, a strong PFT does not cap your rating. Do not let anyone, including a C&P examiner, tell you that normal spirometry ends the analysis. Our guide on preparing for a C&P exam covers how to communicate an episodic condition accurately.
The verified-history rule
DC 6602 carries its own note: in the absence of clinical findings of asthma at the time of examination, a verified history of asthmatic attacks must be of record.
Read that as the regulation admitting what every asthmatic already knows. You may look fine on exam day. The VA wrote the episodic nature of the disease into the code itself, and what carries the claim when the exam is unremarkable is the documented history: ER visits, urgent care notes, in-service sick-call entries for wheezing or shortness of breath, pharmacy refills, pulmonology follow-ups. Every asthma attack that was treated somewhere and never made it into your claims file is evidence the rater will never weigh.
One lung, one rating: the 38 CFR § 4.96 rule
If you also have, or later develop, another respiratory condition such as sleep apnea, COPD, or chronic bronchitis, know this now. Under 38 CFR § 4.96(a), ratings for coexisting respiratory conditions under most respiratory diagnostic codes are not combined. The VA assigns a single rating under the code reflecting the predominant disability, with possible elevation to the next higher level where the overall severity warrants it.
This surprises a lot of veterans who have both asthma and sleep apnea, and it makes the question of which diagnosis controls a strategic one, a decision that is medical before it is legal. We cover the anti-combination rule and the elevation clause in depth in a dedicated guide. If sleep apnea is part of your picture, our analysis of the proposed VA sleep apnea rating change is worth reading alongside it.
Getting service-connected in the first place
The rating tiers above only apply once your asthma is service-connected. Three pathways get you there.
Direct service connection
Asthma diagnosed in service, or linked to service by competent medical evidence. For post-service diagnoses outside the presumptive framework, the medical link is where these claims are won or lost, and where a properly structured nexus letter earns its weight.
Presumptive service connection under the PACT Act
Asthma is on the burn pit presumptive list for veterans with qualifying service. The statute, 38 U.S.C. § 1120, describes it as asthma "diagnosed after service," and asthma is the only one of the 23 listed conditions carrying a timing qualifier. Here is the part almost nobody explains: the regulation VA actually applies today, 38 CFR § 3.320, lists asthma with no timing qualifier at all,³ and in a 2024 proposed rule VA stated plainly that it would implement the presumption without the statutory language, because limiting a presumption to post-service diagnoses conflicts with how presumptions are meant to work.² Which locations and dates qualify, and what this means if you were first diagnosed in service, is covered in our PACT Act asthma guide.
Aggravation
Asthma that existed before service but was permanently worsened beyond its natural progression by service. This is common for veterans who enlisted with waivers or a childhood history, and many of them wrongly assume they are disqualified. If the VA denied you on pre-existing grounds, start with our guide on what to do when the VA denies a pre-existing condition.
Where asthma claims fall short
From the clinical review side, the same gaps appear again and again.
The medication pathway is never argued. The file shows daily Advair, but nothing connects it to the 30% criterion, so the rating rests on a normal PFT. Raters are not required to build your argument for you.
Exacerbations were treated outside the VA. Urgent care steroid bursts are 60% evidence sitting in a civilian records system. Until you submit them, they do not exist for rating purposes.
No verified attack history. The exam is normal, the record is thin, and the rater has nothing to anchor the episodic disease picture the code's own note requires.
The diagnosis itself is contested. Asthma versus COPD versus mixed obstructive disease changes the controlling diagnostic code, and under § 4.96(a) that can change the rating. When the diagnosis is disputed, the specialty of the clinician offering the opinion matters. Our specialty-by-specialty guide explains when a pulmonologist-level opinion is worth it.
Every one of these is fixable with the right documentation before the decision. After the decision, it gets harder.
Get the medication pathway argued correctly
If your asthma rating rests on a breathing test while your prescription history tells a different story, or you are preparing to file and want the DC 6602 criteria mapped correctly the first time, our clinicians do exactly that. A Claim Readiness Review identifies which pathway your evidence already supports and what is missing. When the claim needs the medical link itself, a clinician-authored nexus letter / IMO built around the rating criteria does that job. For increased-rating claims, a DBQ that captures your medication requirements and exacerbation history maps your evidence directly onto the schedule.
Sources
Reddel HK, Bacharier LB, Bateman ED, et al. Global Initiative for Asthma Strategy 2021: Executive Summary and Rationale for Key Changes. American Journal of Respiratory and Critical Care Medicine. 2022;205(1):17-35.
38 CFR § 3.320, Claims based on exposure to fine particulate matter [88 FR 60341, Sept. 1, 2023].
Department of Veterans Affairs. VA Adjudication Regulations for Disability or Death Benefit Claims Based on Toxic Exposure. Proposed rule, 89 FR 79815, October 1, 2024 (RIN 2900-AR75).
38 CFR § 4.97, Diagnostic Code 6602 (Schedule of ratings, respiratory system). eCFR.
38 CFR § 4.96(a) (Special provisions regarding evaluation of respiratory conditions).
38 CFR § 3.320, Claims based on exposure to fine particulate matter [88 FR 60341, Sept. 1, 2023].
38 U.S.C. § 1120 (Presumption of service connection for certain diseases associated with exposure to burn pits and other toxins).
Board of Veterans' Appeals, Citation Nr. A25027831 (March 25, 2025).
Frequently Asked Questions
Yes. The criteria under DC 6602 are connected by "or," so each pathway stands on its own. Daily inhalational anti-inflammatory medication, meaning an inhaled corticosteroid or combination inhaler, independently meets the 30% criteria regardless of your spirometry results. The key is documentation: the prescription and its refill history need to be in your claims file.
It can. Intermittent inhalational bronchodilator therapy is the 10% criterion under DC 6602, so as-needed rescue inhaler use documented in your treatment records supports a compensable rating on its own.
Not if the medication requirement is documented and argued. Under DC 6602 the daily medication requirement is itself the rating criterion, and control achieved through daily treatment is not the same as resolution. A veteran whose asthma is well-controlled on daily Symbicort still meets the 30% criteria through the medication pathway.
Yes, for veterans with qualifying service. The statute describes it as asthma diagnosed after service, but the regulation VA applies today, 38 CFR § 3.320, lists asthma with no timing qualifier, and VA has stated it will not apply the statutory one. The details, including which locations and dates qualify, are covered in our dedicated PACT Act asthma guide.
The regulation requires intermittent courses of systemic (oral or parenteral) corticosteroids at least three times per year. They must be documented and dated in your file. Civilian urgent care and ER records count, but only if they are actually submitted.
Only under conditions. A rating that has been in place for five years or more is considered stabilized under 38 CFR § 3.344 and cannot be reduced without evidence of sustained improvement shown across the full record, and a rating in place for twenty years is protected under 38 CFR § 3.951(b). In practice a reduction requires a re-examination showing genuine, maintained improvement, not one good breathing test on a good day.
It can contribute. Schedular TDIU under 38 CFR § 4.16(a) requires one condition rated at 60%, or a combined 70% with at least one condition at 40%. Severe asthma rated at 60% meets the single-condition threshold on its own, and the claim then turns on evidence that your conditions prevent substantially gainful employment. Our guide on the medical opinion that wins TDIU covers what that evidence looks like.
Unsettled. The 100% criteria include daily use of high-dose systemic corticosteroids or "immunosuppressive medications," and Board decisions have differed on whether asthma biologics fall within that phrase. Outcomes often turn on how the prescribing physician characterizes the medication in the record, which is a question a targeted medical opinion can address directly.
Need help with your VA claim?
Get expert guidance and documentation from our licensed clinicians
Get Free ConsultationEducational Guidance and Evidence Research
View editorial standardsClinical Integrity and Accuracy Review
View medical review policyOriginally published July 17, 2026 • Last updated July 19, 2026
Related Insights
The Proposed VA Sleep Apnea Rating Change: What It Means for Your 50%
ChatGPT Nexus Letter for VA Claims: Why AI-Generated Letters Get Denied and What the VA's 2026 Fraud Tool Means for Veterans
MST Markers: What They Are and How a Psychologist Reads Them
About this article. This post is general educational and medical information published by the Military Disability Nexus clinical team. It is not legal advice, not individualized medical advice, and not a substitute for a personal evaluation by a licensed clinician or a consultation with an accredited representative. Reading it does not create a doctor-patient or attorney-client relationship. VA law and rating criteria change; some details may not reflect the most recent updates, and every claim is decided by the VA on its own facts – no outcome is promised or guaranteed. Military Disability Nexus is an independent medical-evidence provider and is not affiliated with, endorsed by, or acting on behalf of the U.S. Department of Veterans Affairs or any government agency. Free claims assistance is available from VA-accredited Veterans Service Organizations and county Veterans Service Officers; you can verify any representative's accreditation through the VA Office of General Counsel.