What Is a VA Nexus Letter? A Clinician's Anatomy of a Strong Medical Opinion
- 1.What a VA Nexus Letter Actually Is (and Isn't)
- 2.Why the Nexus Is Where Most Claims Stall
- 3.The 5 Elements of a High-Probative Nexus Opinion
- 4.Language That Wins vs. Language That Sinks a Claim
- 5.Nexus Letter vs. C&P Exam: How the VA Weighs Competing Opinions
- 6.Who Should Write Your Nexus Letter?
- 7.5 Mistakes That Destroy Probative Value
- 8.When You Need a Nexus Letter - and When You Don't
- 9.Frequently Asked Questions About VA Nexus Letters
- 10.Your Next Step
What a VA Nexus Letter Actually Is (and Isn't)
A VA nexus letter is a written medical opinion from a licensed healthcare provider that connects your current diagnosed condition to an event, injury, or exposure during your military service. Think of it as an expert witness statement — translated into clinical language — that answers one specific question the VA is asking: "Is this veteran's condition related to their time in service?"
The word "nexus" simply means link. Under 38 CFR § 3.303 (Principles Relating to Service Connection), the VA requires three things before it can grant disability compensation: a current diagnosis, an in-service event, and a medical link between the two. The nexus letter addresses that third element — and it is, by a wide margin, the element that causes the most denials.
What a nexus letter is not: it is not a personal plea, a letter of recommendation, or a recap of your symptoms. It is a structured medical opinion that explains why your condition is connected to service, supported by your records and grounded in clinical reasoning. When written well, it gives the VA's Rating Veterans Service Representative (RVSR) a clear, evidence-based reason to grant service connection. When written poorly, it gives them a reason to deny.
Why the Nexus Is Where Most Claims Stall
Most veterans can point to a current diagnosis. Most can point to something that happened during service. The breakdown happens when no one explains the connection between those two facts in clinical terms the VA can act on.
Consider a veteran who experienced repeated heavy lifting and parachute jumps during airborne training, now diagnosed with lumbar degenerative disc disease fifteen years later. The diagnosis is documented. The service record is clear. But unless a qualified provider walks through the biomechanical reasoning explaining how repetitive axial loading accelerates disc degeneration beyond what age alone would predict the VA rater has no medical basis on which to connect the two. That is the gap a nexus letter fills.
Regulatory Foundation :38 CFR § 3.303(a) states that service connection requires evidence of a disease or injury in service and a present disability, with a rational basis to link the two. 38 CFR § 3.159(a)(1) defines competent medical evidence as evidence provided by a person qualified through education, training, or experience to offer medical diagnoses, statements, or opinions.
The VA processes millions of disability evaluations each year. In that volume, claims without a clear medical nexus often receive negative decisions — not because the connection doesn't exist, but because no one articulated it in the language the adjudication system requires.
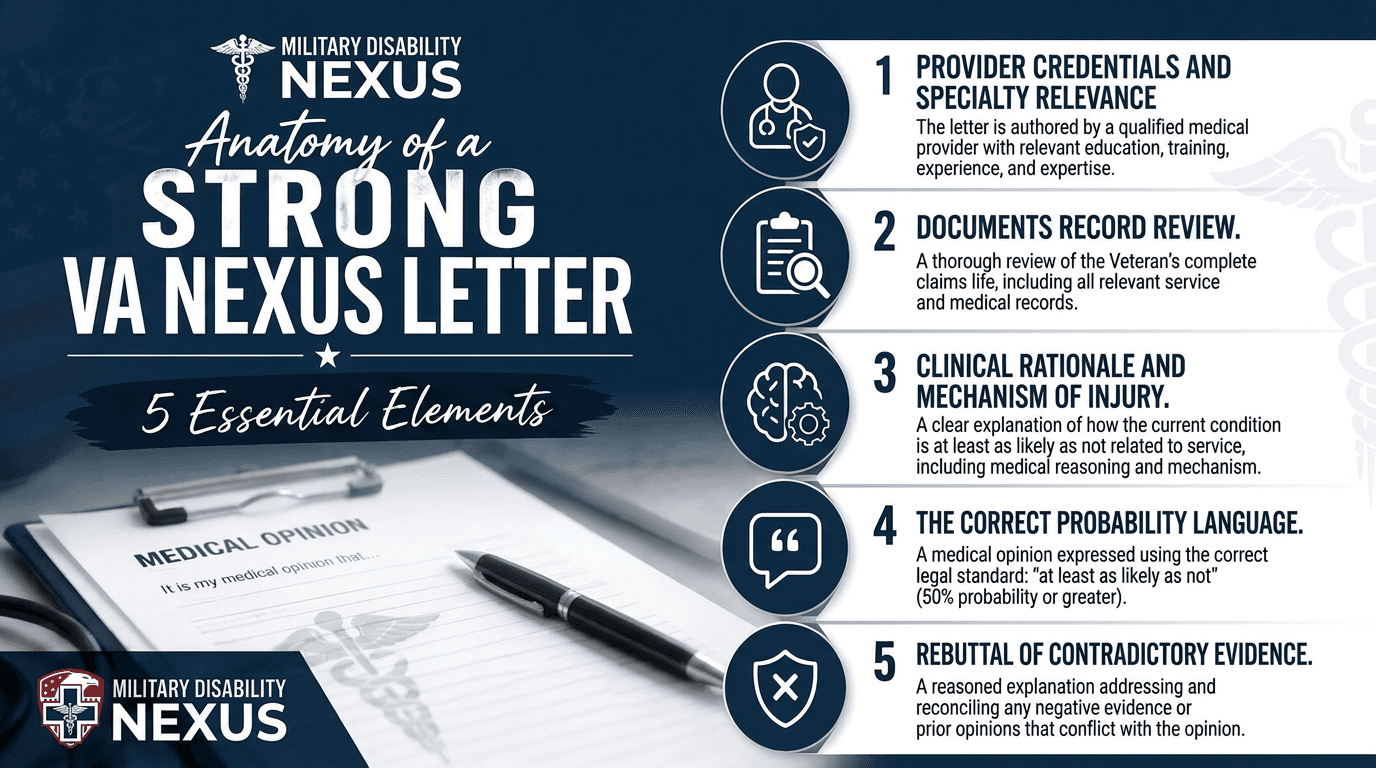
The 5 Elements of a High-Probative Nexus Opinion
Not all nexus letters are created equal. The VA assigns each piece of medical evidence a probative value - essentially, how much weight that evidence carries toward proving (or disproving) a claim. The factors that drive probative value are well-established in case law (see Nieves-Rodriguez v. Peake, 22 Vet. App. 295, 2008) and consistently reinforced in Board of Veterans' Appeals decisions. Here is what a strong nexus opinion contains:
1. Provider Credentials and Specialty Relevance
The letter must identify the authoring clinician's license, board certifications, and area of specialization. A nexus opinion on traumatic brain injury from a board-certified neurologist carries significantly more weight than the same opinion from a general practitioner. The VA specifically uses provider credentials when determining whether an opinion constitutes "competent medical evidence" under 38 CFR § 3.159(a)(1).
2. Documents Record Review.
The clinician must explicitly state which records they reviewed: service treatment records (STRs), post-service medical records, the VA claims file (C-file), relevant imaging or lab results, lay statements, and buddy statements. This is not a formality. In Prejean v. West (13 Vet. App. 444, 2000), the court identified the physician's access to the claims file as a key factor in assessing probative value. A provider who states they reviewed an 850-page C-file sends a fundamentally different credibility signal than one who reviewed "available records."
3. Clinical Rationale and Mechanism of Injury.
This is the backbone of the letter. The provider must explain how the in-service event caused, contributed to, or aggravated the current condition — using accepted medical and scientific reasoning. Strong opinions cite the pathophysiological mechanism (for example, how blast-wave overpressure disrupts neuronal axons, supported by peer-reviewed research such as Goldstein et al., Science Translational Medicine, 2012). An opinion that states a conclusion without explaining the reasoning is treated as a "bare conclusion" and typically receives minimal probative weight.
4. The Correct Probability Language.
The opinion must use VBA-recommended probability language. There are three favorable phrases that meet or exceed the standard — "in all likelihood" (very high confidence), "more likely than not" (greater than 50%), and "at least as likely as not" (50% or greater probability). The last of these is the minimum threshold required to trigger the VA's benefit-of-the-doubt doctrine under 38 U.S.C. § 5107(b). The standard unfavorable phrase is "less likely than not" (below 50%), which is what you will see in most negative C&P exam opinions. The VA's official DMA training for C&P examiners explicitly prohibits speculative language — terms like "might," "may be," "could," or "probably" — because they are too vague to establish a nexus. The U.S. Court of Appeals for Veterans Claims reinforced this in Bostain v. West (1998).
5. Rebuttal of Contradictory Evidence
If a prior C&P exam returned a negative nexus opinion, or if there are gaps in the service treatment records, the nexus letter must address those issues directly. Ignoring contradictory evidence does not make it go away — it tells the VA rater that the clinician either didn't review the full record or couldn't account for the discrepancy. A well-crafted rebuttal — explaining why the C&P examiner's rationale was incomplete, factually inaccurate, or inconsistent with current medical literature — is often the difference between a denial and a grant.
Language That Wins vs. Language That Sinks a Claim
The difference between a granted claim and a denied one often comes down to a handful of words. The table below illustrates why precision in medical-legal language matters:
The VA's DMA (Disability Medical Assessment) training manual prescribes specific VBA-recommended language for C&P examiners. The same language governs how private nexus opinions are evaluated. Here is the complete probability spectrum, from strongest favorable to unfavorable to unacceptable:
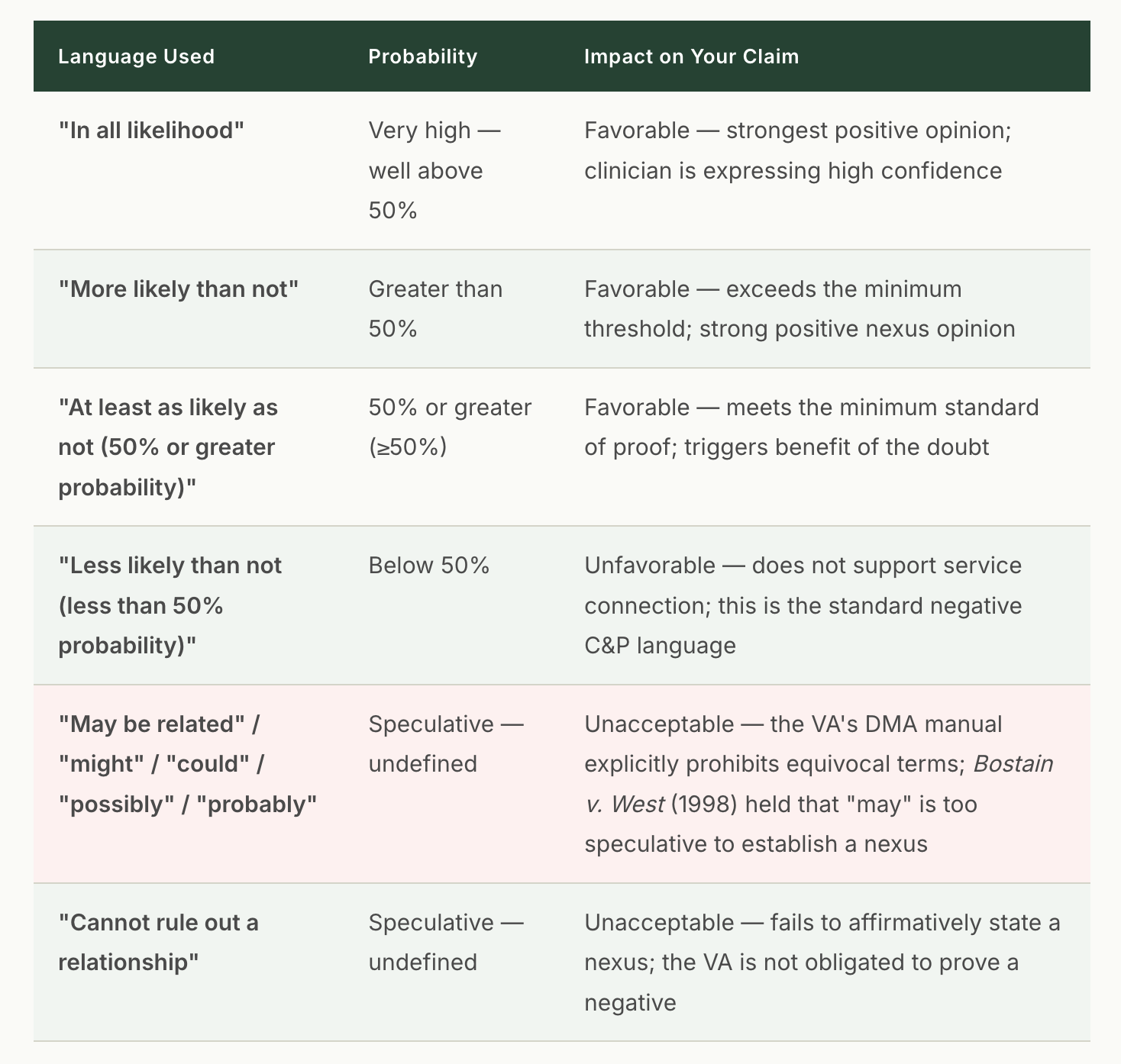
WHY THIS HIERARCHY MATTERS
The three favorable phrases: "in all likelihood," "more likely than not," and "at least as likely as not" - all meet or exceed the VA's standard of proof. "At least as likely as not" is the minimum threshold required. It means the evidence for and against service connection is in approximate balance (50/50), and under the benefit-of-the-doubt doctrine (38 U.S.C. § 5107(b)), the VA must resolve that tie in the veteran's favor.
"Less likely than not" is the standard unfavorable language used by C&P examiners when they determine that the connection to service falls below the 50% threshold. This is the phrase you will see in most negative C&P opinions.
Everything below "less likely than not" — hedging language like "may," "might," "could," or "probably" — is explicitly rejected by the VA's own training materials and by the U.S. Court of Appeals for Veterans Claims. These terms carry no weight and should never appear in a nexus opinion
Source: VA DMA Medical Opinions Training: The VA's official DMA training course for C&P examiners states: "Using equivocal terms such as 'might,' 'may be,' or 'probably' as part of your opinion is unacceptable." The course further instructs examiners to state conclusions using one of two VBA-recommended phrases: (a) "at least as likely as not (50 percent or greater probability)" or (b) "less likely than not (less than a 50 percent probability)." It also notes that examiners may state their degree of certainty in the rationale using additional terms such as "unlikely" or "definitely."
Nexus Letter vs. C&P Exam: How the VA Weighs Competing Opinions
A common misconception is that a C&P (Compensation and Pension) exam "outranks" a private nexus letter. It does not. The VA is required to consider all competent medical evidence of record and must explain its reasoning if it assigns more weight to one opinion over another.
In practice, the VA evaluates competing opinions based on three factors: the provider's qualifications (specialist vs. generalist), the thoroughness of the records review, and the adequacy of the medical rationale. A private nexus letter from a board-certified specialist who reviewed the full C-file and provided a detailed clinical explanation can — and frequently does — outweigh a negative C&P opinion from a generalist who spent fifteen minutes with the veteran and documented a conclusory rationale.
If the two opinions are in approximate balance, the VA must resolve the tie in the veteran's favor under the benefit-of-the-doubt doctrine. This is precisely why the clinical rationale — the "why" behind the opinion — matters so much. A one-paragraph C&P negative opinion that attributes your condition to "the natural aging process" without engaging with your specific service history is vulnerable to rebuttal when a specialist explains why accelerated degeneration patterns in your imaging are inconsistent with age-related changes alone.
Who Should Write Your Nexus Letter?
Any licensed healthcare provider can write a nexus letter. However, the probative value assigned to that opinion depends heavily on the author's credentials relative to your specific condition. A nexus letter about chronic migraines from a board-certified neurologist will generally be weighed more favorably than the same opinion from an internist — not because the internist is unqualified, but because the specialist's training provides deeper authority on the mechanism at issue.
Can a VA doctor write your nexus letter? Technically, yes. Practically, it is rare. VHA Directive 1134(2) requires VA providers to assist with documenting current conditions on forms like DBQs, but it clarifies that VA providers are not expected to make the causality determinations that nexus opinions require. Many VA physicians are explicitly discouraged from writing nexus opinions due to the inherent tension between their employer (the VA) and the veteran's claim against that same employer. For this reason, most veterans obtain nexus letters from independent, private clinicians.
If your treating physician is willing to write the letter, that can be a strong option — a long-standing clinical relationship carries its own credibility. However, the provider must still follow the structure outlined above. A heartfelt letter from your doctor that says "I've treated this veteran for years and believe their condition is related to service" without a documented records review, clinical rationale, and proper probability language will not carry the weight you need.
5 Mistakes That Destroy Probative Value
Through hundreds of clinical record reviews (CRRs), our team sees the same patterns in nexus letters that fail. Understanding these mistakes can save you months — or years — in the appeals process.
Mistake 1: The Template Letter
Generic, one-page nexus letters that could apply to any veteran with any condition are immediately identifiable to experienced VA raters. If the letter doesn't reference your specific service history, your specific diagnosis, and your specific records, it signals that the clinician invested minimal effort — and the VA will weigh it accordingly.
Mistake 2: Missing the Mechanism
Stating "the veteran's lumbar condition is at least as likely as not related to service" without explaining the biomechanical, physiological, or clinical pathway is a bare conclusion. Peer-reviewed literature supports the explanation. For example, research published in The Spine Journal has demonstrated that repeated high-impact axial loading — common in military occupational specialties involving parachute landings, heavy vehicle operation, and load-bearing marches — accelerates disc degeneration beyond age-matched civilian controls (Spine J., Knox et al., 2014). That kind of citation gives the rater something concrete to evaluate.
Mistake 3: Using Speculative or Equivocal Language
As shown in the comparison table above, language matters enormously. The opinion must use one of the three favorable phrases: "in all likelihood," "more likely than not," or "at least as likely as not." The VA's DMA training explicitly labels hedging terms like "might," "may be," "could," and "probably" as unacceptable. Even the word "probably" — which sounds favorable to most people — is considered too equivocal for VA adjudication purposes. If your nexus letter uses any of these speculative phrases instead of the VBA-recommended language, the VA can disregard the opinion entirely.
Mistake 4: Ignoring the Negative C&P Opinion
If the VA already has a C&P exam on file that concluded "less likely than not," your nexus letter must engage with that opinion directly. Explain what the C&P examiner got wrong, what records they didn't review, or what medical reasoning they failed to apply. A nexus letter that pretends the negative opinion doesn't exist is asking the VA to do the rebuttal work for you. They won't.
Mistake 5: Wrong Credentials for the Condition
A psychiatrist writing a nexus opinion for a complex orthopedic condition - or a podiatrist opining on PTSD -creates an immediate credibility problem. The provider's specialty should match the condition being evaluated. When it doesn't, the VA can reasonably assign the opinion lower probative weight, regardless of how well-written the rationale is.
When You Need a Nexus Letter - and When You Don't
Not every VA claim requires a nexus letter. Here is how to know whether your case needs one:
You likely need a nexus letter if: your condition developed after service and the connection isn't obvious from your records; you're filing a secondary service-connection claim (where a service-connected condition caused or aggravated a new condition); your initial claim was denied for "no nexus"; a C&P exam returned a negative opinion; or your service treatment records are incomplete or don't document the in-service event.
You may not need a nexus letter if: your condition falls under a VA presumptive category (such as Agent Orange conditions under 38 CFR § 3.309(e), PACT Act burn pit presumptives, or Gulf War undiagnosed illness under 38 CFR § 3.317); you have continuous, well-documented treatment from service to the present with no break; or the in-service injury and current diagnosis are the same condition with clear continuity in your records.
When Presumptive Claims Still Need a Nexus: If your condition is not on the specific presumptive list — or if the VA denies your presumptive claim — you may still establish service connection through a direct nexus opinion. For example, a veteran exposed to burn pit emissions who develops a respiratory condition not currently listed as a PACT Act presumptive may still succeed with a strong nexus letter tying that specific exposure to that specific diagnosis.
Need a Nexus Letter That Meets the Standard?
Our clinical team writes evidence-based nexus opinions grounded in your records, your service history, and current medical literature — built to carry probative weight with VA raters.
Frequently Asked Questions About VA Nexus Letters
What is a VA Nexus Letter?
A VA nexus letter is a written medical opinion from a licensed healthcare provider that connects your current diagnosed condition to an event, injury, or exposure during your military service. It addresses the "nexus" (link) requirement for service connection under 38 CFR § 3.303. The opinion must reach the "at least as likely as not" standard — a 50% or greater probability that your condition is related to service.
Can any doctor write a nexus letter for a VA Claim?
Any licensed healthcare provider can technically write one. But specialists in the relevant medical field carry more probative value with VA raters. An orthopedic surgeon's opinion on a knee condition will generally outweigh a family medicine physician's opinion on the same condition — because of the depth of training in that specific area. The provider must also demonstrate familiarity with your full medical and service history.
Can a VA Doctor write a nexus letter?
VA-employed physicians face significant limitations. VHA Directive 1134(2) requires VA providers to assist with medical documentation like DBQs, but clarifies they are not expected to make the causality determinations nexus letters require. Due to potential conflicts of interest, most VA doctors are discouraged from writing nexus opinions. Veterans typically obtain these from independent, private providers.
How much does a nexus letter cost?
Costs generally range from $500 to $2,500, depending on the complexity of the condition, the provider's specialty credentials, and whether a records review or examination is included. Prices under $300 often signal template-based, low-effort opinions with minimal probative value. Prices over $3,000 should be justified by the provider's credentials or the case complexity. Most veterans recover their nexus letter costs within the first month or two of receiving compensation..
What does "at least as likely as not" mean?
It is the VA's legal standard of proof - a 50% or greater probability that the condition is connected to service. This is far lower than criminal court's "beyond a reasonable doubt." When the evidence for and against service connection is roughly equal, the VA must decide in the veteran's favor under the benefit-of-the-doubt doctrine (38 U.S.C. § 5107). Language weaker than this standard - "might be related," "could be connected" — is typically insufficient..
My claim was denied even with a nexus letter. What went wrong?
The most common reasons: the letter used speculative language instead of "at least as likely as not"; the author lacked relevant specialty credentials; the letter didn't document a thorough records review; the clinical rationale was too vague or conclusory; or the letter failed to address a contradictory C&P exam opinion. A Supplemental Claim with a stronger, more detailed nexus opinion -one that directly rebuts the reasons for denial - can often overcome these issues.
What is the difference between a nexus letter and a C&P Exam?
A C&P exam is ordered by the VA and conducted by a VA-contracted examiner. A nexus letter is a private medical opinion obtained independently by the veteran. Both carry evidentiary weight. If a C&P exam returns a negative opinion, a private nexus letter can serve as competing evidence. The VA must weigh both based on probative value - the provider's credentials, the completeness of their review, and the strength of their rationale.
Do I need a nexus letter for a presumptive condition ?
Generally, no. Presumptive conditions (Agent Orange, PACT Act burn pits, Gulf War illness, Camp Lejeune water contamination) do not require additional proof of a nexus - the VA presumes the connection. But if your presumptive claim is denied, or your specific condition is not on the presumptive list, a nexus letter establishing a direct service connection may be necessary.
Your Next Step
If your claim was denied for lack of a nexus, if your C&P exam returned a negative opinion, or if you are filing a new claim and want to lead with strong evidence - the next step is a Clinical Record Review (CRR). Our clinical team will review your records, identify evidentiary gaps, and determine whether a nexus letter, a DBQ, or both will best support your claim.
Need help with your VA claim?
Get expert guidance and documentation from our licensed clinicians
Get Free ConsultationDr. Kishan Bhalani is a subject matter expert on VA disability claims documentation, with more than five years of focused work at the intersection of clinical m…
Dr. Kishan Bhalani is a subject matter expert on VA disability claims documentation, with more than five years of focused work at the intersection of clinical m…
Originally published May 1, 2026 • Last updated May 3, 2026
Related Insights
Is Your VA Claim Really Ready to File?
Who Should Write Your VA Nexus Letter? A Clinician's Specialty-by-Specialty Guide (2026)
Can PTSD Cause Migraines? The Clinical Case for Migraines Secondary to PTSD
About this article. This post is general educational and medical information published by the Military Disability Nexus clinical team. It is not legal advice, not individualized medical advice, and not a substitute for a personal evaluation by a licensed clinician or a consultation with an accredited representative. Reading it does not create a doctor-patient or attorney-client relationship. VA law and rating criteria change; some details may not reflect the most recent updates, and every claim is decided by the VA on its own facts – no outcome is promised or guaranteed. Military Disability Nexus is an independent medical-evidence provider and is not affiliated with, endorsed by, or acting on behalf of the U.S. Department of Veterans Affairs or any government agency. Free claims assistance is available from VA-accredited Veterans Service Organizations and county Veterans Service Officers; you can verify any representative's accreditation through the VA Office of General Counsel.