Crohn's Secondary to PTSD VA Claim: Why It Gets Denied
- 1.If You're Reading This, You're Probably Frustrated
- 2.Can You Get VA Disability for Crohn's Disease Secondary to PTSD?
- 3.The Medical Link Between PTSD and Crohn's Disease
- 4.Why most Gastroenterologists Won't Write You a Nexus Letter
- 5.Why Most Nexus Letters for Crohn's Secondary to PTSD Get Rejected
- 6.What a VA-Compliant Nexus Letter Actually Needs
- 7.If You've Already Been Denied: You Have 365 Days
THE SHORT ANSWERCrohn's disease can be service-connected as secondary to PTSD. The medical link between chronic PTSD and inflammatory bowel disease is well documented in peer-reviewed research. But most of these claims get denied - not because the connection isn't real, but because the nexus letter didn't prove it the way VA raters are required to accept. The fix is a properly structured medical opinion that covers causation, aggravation, and the specific gut-brain mechanisms linking PTSD to Crohn's..
If You're Reading This, You're Probably Frustrated
Maybe your VA gastroenterologist told you they "can't" write a nexus letter. Maybe your civilian GI said it was "outside their scope." Maybe you already filed, already went through the C&P exam, and got back a denial letter that told you there wasn't enough medical evidence even though you've had Crohn's for over a decade, had a colectomy, deal with chronic anemia, and live with symptoms nobody should have to explain to a stranger.
You're not imagining it. This is one of the most common dead-ends in the VA claims process: a veteran with an obvious medical condition, a clear timeline, and no doctor willing to put the connection in writing.
Your doctors aren't wrong. They're just not trained for this. Treating Crohn's is one job. Writing a legally sufficient medical opinion to the VA's evidentiary standard is a completely different one.
That's the gap. And it's why these claims keep getting denied.
Can You Get VA Disability for Crohn's Disease Secondary to PTSD?
Yes. Under 38 CFR § 3.310, the VA grants service connection for any condition that is caused or aggravated by an already service-connected disability. If your PTSD is service-connected and there is sound medical evidence that it caused or worsened your Crohn's disease, you are entitled to a secondary service connection rating.
Crohn's disease is rated under 38 CFR § 4.114, diagnostic code 7323, with ratings of 10%, 30%, 60%, or 100% depending on severity, frequency of flares, weight loss, anemia, and functional impact.
The Medical Link Between PTSD and Crohn's Disease
PTSD doesn't just live in your head. It changes how your body works especially your gut. Here's what the science actually shows, without the jargon.
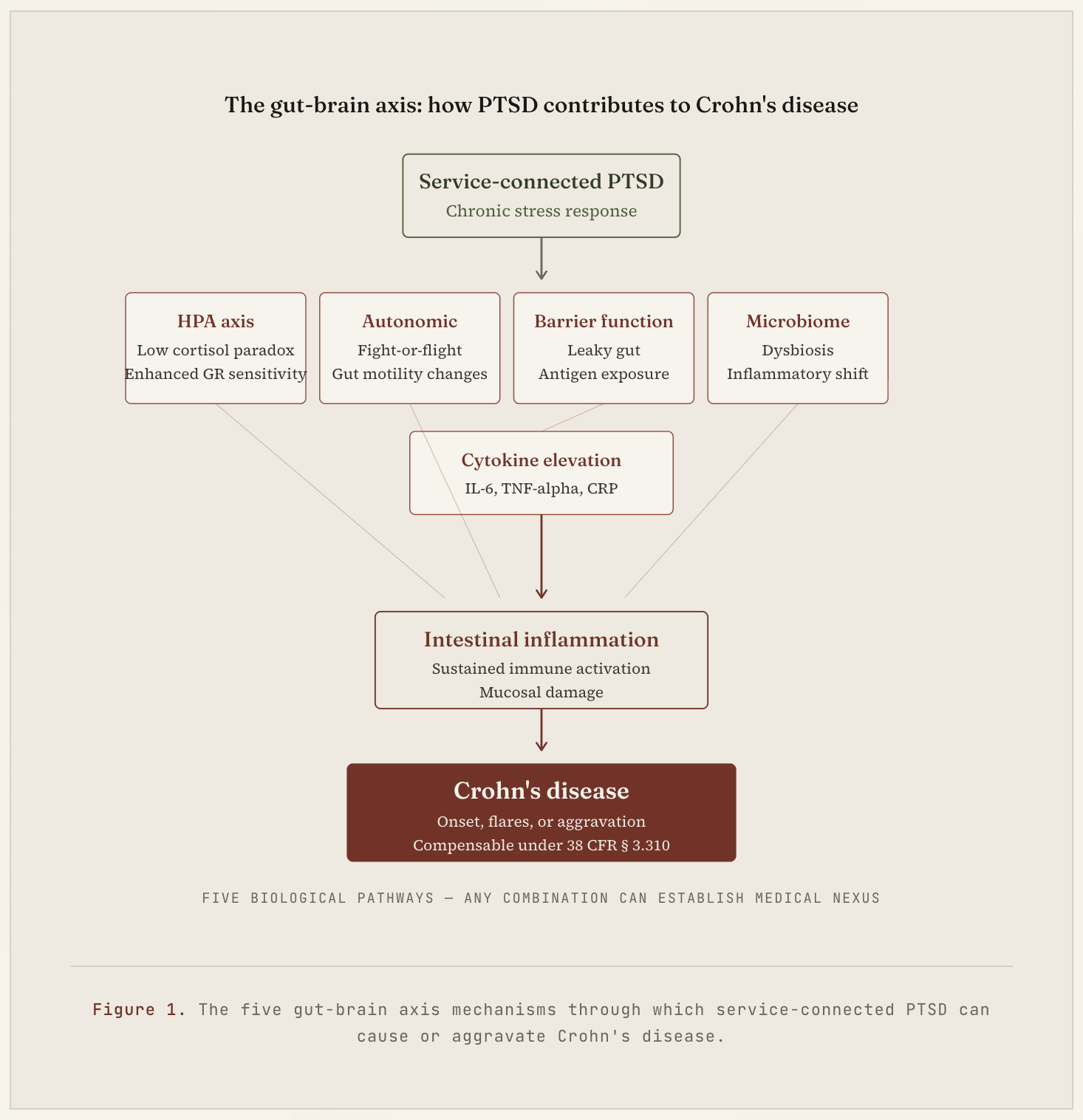
The stress hormone system gets stuck in a dysfunctional loop
Here's a finding that surprises most people: in chronic PTSD, cortisol levels are actually low, not high. Researchers call it the low cortisol paradox, and it's been replicated across decades of studies in combat veterans and other trauma populations.
The mechanism is subtle but important. PTSD causes the body's cortisol receptors to become hypersensitive. The system overcorrects pulling cortisol levels down below normal and keeping them there. Because cortisol is your body's main natural anti-inflammatory hormone, low cortisol means nothing is braking inflammation the way it should. The result is a chronic low-grade inflammatory state the body can't shut off - the opposite of what you'd expect, and exactly why PTSD drives inflammatory diseases like Crohn's.
Your nervous system gets stuck in fight-or-flight
PTSD keeps the sympathetic nervous system on high alert long after the threat is gone. That chronic overactivation changes how your intestines move, how much blood flows through them, and how well the gut lining stays intact — all measurable in PTSD populations.
The gut lining starts to leak
A 2022 study in veterans with PTSD found significantly elevated LPS and LBP two markers of intestinal barrier dysfunction compared to matched controls. In plain English, the gut lining becomes more permeable. When that happens, the immune system starts reacting to bacteria and food particles that shouldn't be crossing the barrier, triggering the exact kind of inflammation seen in Crohn's.
The gut bacteria shift toward inflammation
PTSD cohorts consistently show dysbiosis - a reduction in anti-inflammatory bacteria like Faecalibacterium prausnitzii and Bifidobacterium, and a shift toward species that promote inflammation. The same bacterial imbalances show up in Crohn's disease, which is part of why the two conditions amplify each other.
Inflammatory markers run high
PTSD populations show sustained elevation of IL-6, TNF-alpha, IL-1β, and CRP — the same inflammatory chemicals that drive Crohn's flares. In the Swiss Crohn's cohort study, patients with PTS symptoms had 13 times higher odds of disease exacerbation than patients without PTS — a finding that's hard to explain without a shared inflammatory mechanism.
Clinical Note
Every one of these mechanisms has published research behind it. This isn't a theory someone made up to win a claim — it's established medicine.
Why most Gastroenterologists Won't Write You a Nexus Letter
This is probably the most frustrating part. You go to your GI, show them your service-connected PTSD rating, ask for a nexus letter — and get told no. Here's what's actually happening:
VA doctors are discouraged (and sometimes internally prohibited) from writing opinions on service connection. Civilian GIs don't know the "at least as likely as not" legal standard. Most doctors aren't familiar with the specific VA rating rules. Writing a defensible nexus opinion requires legal-medical training most clinicians never received. And a badly written letter can actually hurt your claim so cautious doctors decline.
None of this means your claim isn't valid. It just means the person qualified to diagnose you isn't the right person to write your VA opinion. Those are two different jobs.
Why Most Nexus Letters for Crohn's Secondary to PTSD Get Rejected
We've reviewed a lot of denied Crohn's-to-PTSD claims. The same patterns show up again and again.
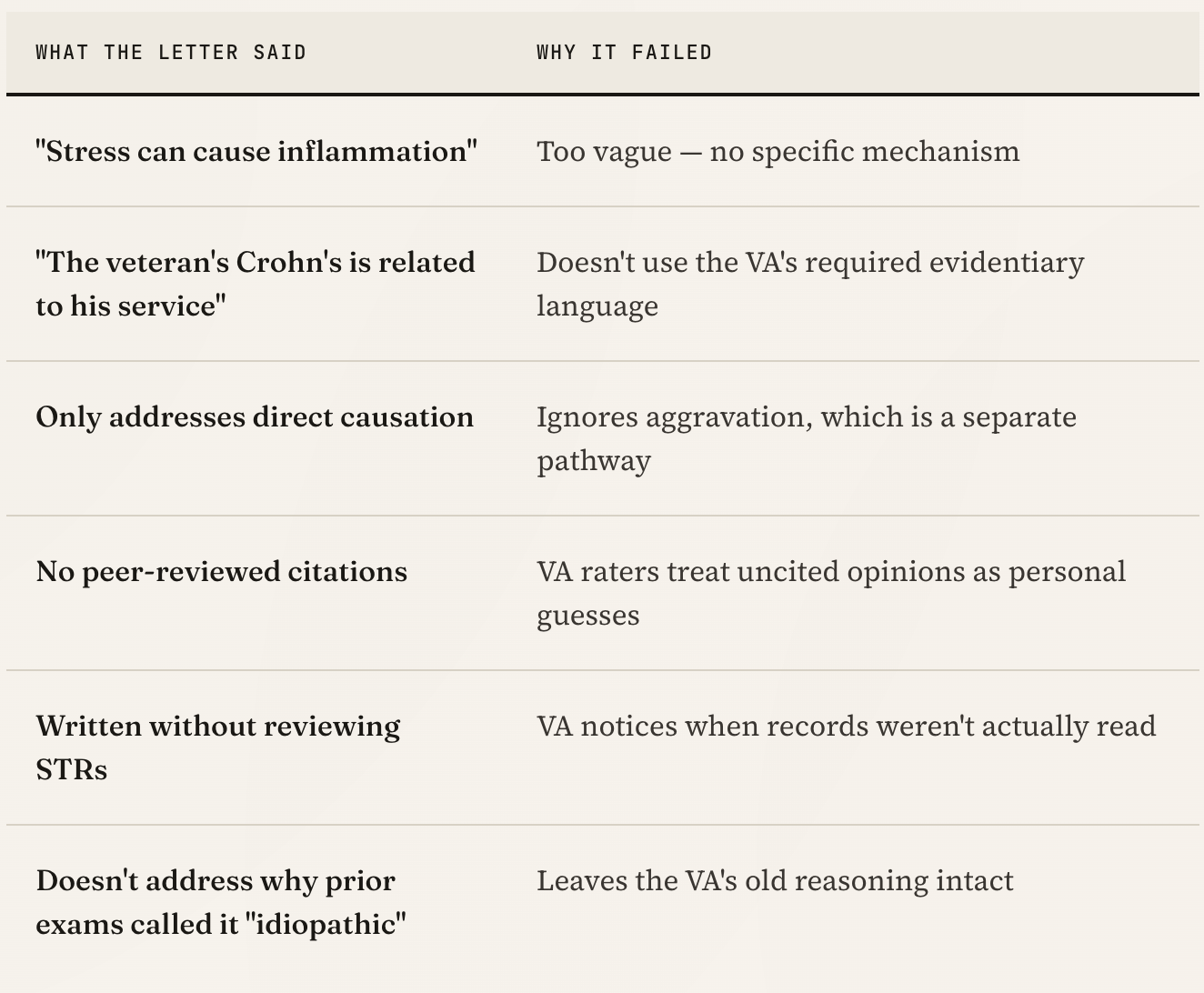
If your denial letter used phrases like "insufficient medical nexus," "not shown to be related to service," or "no causal link established" — one of the issues above is almost certainly why.
What a VA-Compliant Nexus Letter Actually Needs
A nexus letter that survives VA scrutiny for Crohn's secondary to PTSD has to do six specific things.
01
Show the clinician reviewed your full record
Service treatment records, post-service GI workups, pathology, operative reports, current treatment notes. A letter that only references a summary intake gets weighed accordingly. VA raters notice when an opinion references specific records.
02
Use the exact phrase "at least as likely as not"
This is the VA's 50%-or-greater evidentiary standard. Without this language applied to the specific question being answered, the opinion fails on procedure alone.
03
Walk through the specific biological mechanism
"Stress causes inflammation" is not enough. The opinion must name the HPA axis, autonomic changes, barrier function, microbiome, cytokines — and explain how each applies to this veteran's presentation.
04
Cite peer-reviewed medical literature
This transforms the opinion from a personal view into an evidence-based analysis. Raters weigh cited opinions far more heavily.
05
Address aggravation, not just causation
Even when direct causation is debatable, aggravation often is not. Under 38 CFR § 3.310(b), PTSD worsening the natural course of Crohn's is a separately compensable pathway.
06
Rebut the reasoning from any prior denials
If a previous exam called your Crohn's "idiopathic" or "unrelated," the new opinion has to take that argument on directly — not ignore it.
If You've Already Been Denied: You Have 365 Days
A denial is not the end of the claim. You have one year from the decision date to file a Supplemental Claim with new and relevant evidence and a properly constructed nexus opinion is, by definition, new and relevant evidence.
Preserving your effective date within that one-year window is often worth tens of thousands of dollars in retroactive benefits. For a 60% Crohn's rating, that can mean significant back pay depending on how long the claim has been pending.
Before you file anything else, read your denial letter carefully. The VA is required to tell you exactly why they denied the claim. That reasoning is your blueprint for what the next submission has to fix.
Questions Veterans Actually Ask (FAQ)The questions below are the ones that come up most often in our discovery calls - the specific fears, confusions, and "is this even worth it" moments veterans hit when they start looking at a Crohn's secondary to PTSD claim.
Can PTSD actually cause Crohn's disease?
Yes, the medical literature supports a real causal relationship. Chronic PTSD drives HPA-axis dysregulation, sympathetic overactivation, intestinal barrier dysfunction, microbiome disruption, and elevated inflammatory cytokines. Every one of these is independently linked to Crohn's onset and flare activity in peer-reviewed gastroenterology and neuroimmunology research.
Crohn's is multifactorial, but PTSD is a medically defensible cause or aggravating factor — and the VA recognizes both pathways under 38 CFR § 3.310.
What if my Crohn's started before my PTSD was rated?
You may still qualify under the aggravation pathway in 38 CFR § 3.310(b). Aggravation means your service-connected PTSD has made your existing Crohn's worse than its natural progression - more frequent flares, reduced treatment response, accelerated complications.
This is a separate, independently compensable pathway from direct causation. A strong nexus opinion should always analyze both, because aggravation often succeeds when causation is borderline.
I already get 70% for PTSD. Will adding Crohn's actually change my rating?
In most cases, yes. Crohn's is rated separately under diagnostic code 7323 at 10%, 30%, 60%, or 100%. The VA combines ratings using its combined ratings table (not simple addition), so a 70% PTSD rating plus a 60% Crohn's rating combines to roughly 88% — which rounds to 90%.
A separate Crohn's rating may also open the door to TDIU, SMC, or 100% combined eligibility depending on your overall disability picture.
My PTSD is service-connected but not "combat-related." Does that matter?
No. For a secondary service connection claim, the only thing that matters is that your PTSD is already service-connected. Whether it was granted through combat stressors, MST, training accidents, or non-combat traumatic events is irrelevant to the Crohn's-secondary analysis.
The medical question is whether PTSD as it exists in your body caused or aggravated the Crohn's. The origin of the PTSD doesn't change the physiology.
What medical records do I need to support this claim?
The strongest Crohn's-to-PTSD files include: your service treatment records (showing any GI-related sick call visits or symptoms), PTSD treatment history including therapy and medication records, GI workup documentation (colonoscopy, imaging, pathology, operative reports), and current treatment notes showing active disease.
You don't need every record perfectly organized — a qualified clinician can work with what you have and tell you what gaps matter.
I didn't have GI symptoms during service. Does that kill my claim?
No, not for a secondary claim. Direct service connection would require in-service symptom onset, but secondary service connection works differently. The legal question is whether your service-connected PTSD caused or aggravated Crohn's - and that disease process can develop years after discharge.
Many successful Crohn's-secondary-to-PTSD claims involve veterans whose gut symptoms emerged 5, 10, or 20 years post-service, well after PTSD was established.
What makes a nexus letter strong enough to survive VA review?
Six things: (1) full record review, not a summary intake; (2) the exact phrase "at least as likely as not" applied to the right question; (3) specific mechanistic rationale covering HPA axis, autonomic function, barrier dysfunction, microbiome, and cytokines; (4) peer-reviewed citations; (5) both causation and aggravation analysis; (6) direct rebuttal of any prior denial reasoning.
A letter missing any one of these is often weighed lightly by raters even if the underlying medical opinion is correct
My claim was just denied. What's my first move?
Read the denial letter before doing anything else. The VA is legally required to tell you exactly why the claim was denied — that reasoning is your blueprint for what to fix.
Next, note your decision date. You have 365 days to file a Supplemental Claim with new evidence while preserving your effective date (and back pay). Don't rush into an HLR or Board appeal until you know which lane the denial actually fits.
Do I need a lawyer or VSO for this?
Not necessarily. For a Crohn's-secondary-to-PTSD claim, the deciding factor is almost always the medical evidence, not the filing process itself. Many veterans succeed at the Supplemental Claim level with a strong nexus opinion and nothing else.
A VA-accredited attorney or agent becomes more valuable at the Board of Veterans' Appeals level or when procedural errors are involved. We don't file claims - we build the medical record.
What if I pay for a nexus letter and still get denied?
Fair concern — and one of the reasons we review records before accepting a case. If the evidence doesn't support a defensible opinion, we tell you upfront rather than take your money and write a weak letter.
If a claim is denied after a properly structured opinion, the letter still becomes part of your permanent file and supports future Supplemental Claims, HLRs, or Board appeals. Good medical evidence compounds across filings — it isn't wasted.
? Still have a question we didn't answer?
If your situation has a twist these answers don't cover - a specific denial reason, an unusual timeline, a pre-existing condition question - a short discovery call is the fastest way to get a clinical read on it. No sales pitch, no pressure.
Need help with your VA claim?
Get expert guidance and documentation from our licensed clinicians
Get Free ConsultationEducational Guidance and Evidence Research
View editorial standardsClinical Integrity and Accuracy Review
View medical review policyOriginally published April 20, 2026 • Last updated May 3, 2026
Related Insights
PTSD VA Disability Claim: Nexus Letters, Denial Reasons & Your Complete Filing Guide
Is Your VA Claim Really Ready to File?
Asthma VA Rating Explained: How DC 6602 Actually Works (And Why a Normal Breathing Test Doesn't Cap Your Rating)
About this article. This post is general educational and medical information published by the Military Disability Nexus clinical team. It is not legal advice, not individualized medical advice, and not a substitute for a personal evaluation by a licensed clinician or a consultation with an accredited representative. Reading it does not create a doctor-patient or attorney-client relationship. VA law and rating criteria change; some details may not reflect the most recent updates, and every claim is decided by the VA on its own facts – no outcome is promised or guaranteed. Military Disability Nexus is an independent medical-evidence provider and is not affiliated with, endorsed by, or acting on behalf of the U.S. Department of Veterans Affairs or any government agency. Free claims assistance is available from VA-accredited Veterans Service Organizations and county Veterans Service Officers; you can verify any representative's accreditation through the VA Office of General Counsel.